

Summary
The incidence of laryngotracheal trauma has been decreased after seat belt usage. Laryngeal and tracheal trauma encompasses less than 1 % of trauma in biggest centers of trauma in North America and Europe.
Forensic trauma may threaten life and quality. Insertion of life important structures of respiratory system branches of vascular system, digestive organs, peripheral nerves or central system, obligate us to treat it very carefully and in collaboration with other structures to assume high quality in treatment of possible damages in cases that we manage.
Key words
- Laryngeal
- Injury
- Tracheotomy
- Treatment
Observation
The paper is a case study. L.T 26 years old, underwent a car crash accident, while he was driving a motorbike. The patient was sent to our hospital in the emergency unit.
On the first evaluation he was alert, but presented symptoms of extended contusion of the anterior neck region, associated with a deep horizontal cut at the supralaringeal level. The extend of the wound was approx 5 cm. The patient was bleeding and had breathing difficulties.
The paper describes the preoperatory evaluation, the surgical treatment and the follow up of the patient. The conclusion is that patients with laryngeal trauma must receive emergent treatment as tracheotomy and carefully inspection and reconstruction of entire larynx in order to save lives, than to be started follow-up phonetic and speech therapy as early as possible.
Résumé
L’incidence de traumatisme de laryngotracheal a été diminuée après l’usage de ceinture de sécurité. Traumatisme laryngé et trachéal entoure moins que 1 % de traumatisme dans les plus grands centres de traumatisme en Amérique du Nord et Europe. Le traumatisme légal peut la vie en menace et diminue la qualité. L’insertion de vie structures importantes de branches de système respiratoire de système vasculaire, les organes digestifs, les nerfs de périphérique ou le système central, nous obligent de le traiter très soigneusement et dans la collaboration avec les autres structures pour supposer la qualité supérieure dans le traitement de dommages possibles dans les cas que nous gérons.
Case presentation
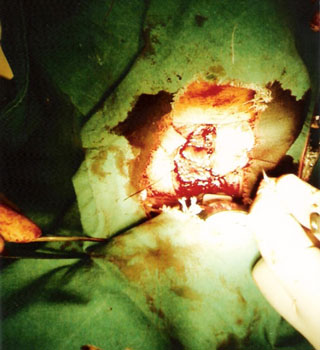
Patient LT 26 years old was crashed from a car during travelling by motorbike. He was transported urgently in emergency of central military hospital. First evaluated patient was alert, but he presented clear evidence of massive contusion during all anterior hyoid thyroid regions, accompanied of a deep horizontal cut of 5 cm, which was bleeding. Patient suffered of breathing difficulties. (Fig 1)
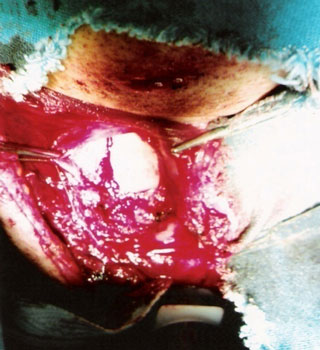
Immediately the patient was placed under mask oxygenation (Fig 1). Second step was stabilizing of airways. Because he presented damage of neck kind of contusion, bleeding and laryngeal trauma in a not known extent, we decided to perform emergency tracheotomy and not intubation. (Fig 2)
Tracheotomy was difficult because of extent of damage and inabilitty of neck deflection. We exposed the 3 and 4 tracheal ring, and removed 1/3 anterior of 4 (Fig3). After performing tracheotomy and stabilising airways we prolonded the incision until to horizontal cut level for a complete evaluation of damages of laryngeal block. During examination resulted dissection of soft tissues until hypofarings level, accompagnied to vertical fracture of thyroid cartilage without rupture of endolaryngeal mucosal, but with displacement of two thyroid cartilage parts (Fig4). We noticed contusive damage of muscles and hypodermal tissue that started from hyoid region and continuing to first tracheal rings (Fig5).
In order to evaluate the situation of internal part of airways, during direct laryngoscopy, we noticed visible endolaringeal hematoma of vocal cords and swelling but not rupture of internal mucosa.
Elaboration of damaged structures was realized from inside out adjoining and sewing thyroid cartilage and pericondrum together (after leaving apart little chopped pieces of thyroid cartilage.
The wound was sewed in straits (Fig 6).
Breathing in next days would be realized via tracheotomy, this made possible primary healing of the wound.
At 6 Th days, after removal of tracheotomy tube, patient has free breathing but is dysphonic(Fig7). During endoscopic examination of larynx 3 weeks after the intervention we noticed that hematomas in vocal cords were disappeared, despite persisting hyperemia and a little disproportion of length of vocal cords(Fig 8).
Also we noticed a slight edema of anterior commissural of larynx. Mobility of structures was preserved.
Patient was presented for next control 2 months after submitting trauma. in the neck the cicatrix was remarkable in T shape, but excluding a slight harsh voice the patient didn’t present other complains (Fig9).
Discussion
Despite car accidents are increased during last 15 years in our country damages of laryngeal and tracheal block are not frequent, because mandible arc serves as a natural barrier of larynx, and for more it is not ENT doctor who came across this situation, but equips of emergency services.6, Even when this kind of trauma appear as mild cases they are under evaluated, but consequences are severe. 2,3,6
Either vocal function is not evaluated from emergency unit. We will not treat the mechanism of damaging, but discussing our case we have combined penetrate damage and blunt damage over thyroid cartilage. The last one is a consequence of crashing laryngeal and tracheal block over vertebral colonna, so laryngeal and tracheal damages will be in proportion to crush pressure. 4,5,6,7. In our case patient neck was smashed next to the edge of pavement.
Let s go back to first evaluation. Establishment and maintenance of the airways is the utmost urgency in treating any neck injured patient with trauma. 1,2,3,6,8
Surgeon asses breathing, but also look for intubation as a solution which is a contraindication for ENT doctor. Because intubation is difficult in a larynx with edema and hemorrhage, and may damage more laryngeal structures already damaged from trauma. ENT doctor has as a priority tracheotomy, than intubation. He can work freely to larynx, as presented in our case.1, By the way we have to admit that this problem in children become more difficult.
Particularities in children s neck trauma.6,7,8
Breathing difficulties is more frequent compared to adults according to the same damage.
- Laryngeal lumen is narrower.
- Soft tissues are more vulnerable and they can swell easily.
- Larynx is in higher position and more protected (mandible arc).
Patients that don’t have breathing difficulties are kept under observation and other examinations and detailed anamnesis are carried out.
Diagnosis is not difficult but we have to deal with an open wound, so far the control of the damage on the wound it has not to be carried out of intervention room, because the control of the wound out of it may open any haemorrhage source complicating more the situation. In an extreme emergency after breathing settling, the wound must be open further in order to control other tissues, as we acted in our case.6, If we have to deal with a non open wound will evaluate voice quality, throat pain especially in swallowing, dyspnoea, subcutaneous emphysema, stridor, etc.1,3,4,6
If the situation is stable we can perform direct or indirect laryngoscopy, fibrolaringoscopy and CT in order to evaluate condition of cartilage skeleton of laryngeal and tracheal block.2,4,6
The damage of larynges tracheal block is categorized in 4 degree. 1,3
- First degree. Visible endolaryngeal hematoma without swelling. Fracture of hyoid bone. No fracture of the cricoids or thyroid cartilage.
- Second degree .Visible endolaryngeal as the hematoma or swelling. Vocal cord dysfunction. Detectable, immobile fracture of cricoids or thyroid cartilage.
- Third degree. Free endolaryngeal cartilage. Unstable fracture of the cricoids or thyroid cartilage.
- Forth degree. Open laryngeal injury. Laryngotracheal separation.
Without any doubt our case is classified in 3 the group (instability of thyroid cartilage). As far as concerned the treatment patients of the 1 and 2 group must be kept under observation as in patients. I.v administration of 1000 mg prednisolone,500mg for children, inhalation with microephinephrine, possibly intensive care observation, consider early intubation before complication occur. In cases with lacerations of the mucosal is counseled placement of nasal gastric and anti reflux drugs, antibiotics.1,2,3
In 3 and 4 type injury of the laryngeal skeleton can be treated with sutures placed through the cartilage or with miniplates. Any fracture must be fully explored. After treating intralayingeal injuries, thyroid cartilage can be reconstructed (from inside out) counseled surgical intervention with reconstruction of cartilage frame as much as possible and placement of the stent.
Tracheotomy as first intervention is recommended in all ages. 1,2,4,5,6
Patients with laryngeal trauma at first sight may seem normal. This fake view augment the risk for a wrong diagnose which results in a bad management, which results in serious problem of airways and phonetic dysfunction.1,6,7,8
Conclusions
Early tracheotomy can avoid hasty and less meticulous management occurring with respiratory distress.
Neck injury can continue to bleed into the soft tissues, causing respiratory distress. All wound tracts must therefore be explored and expose, even if they unremarkable.
Patients with laryngeal trauma must receive follow-up phonetic and speech therapy as early as possible.







References:
1. Arne Ernst, Michael Herzog, Rainer O.Seidl. Head and neck trauma, Thieme Stuttgart 2006, 2-6, 205-208.
2. Charles W.Cummings, John M.Fredrickson, Charles J. Krause, David E.Schuller. Otolaryngology head and neck surgery. Mosby Year Book, St.Louis, Missouri 1993, 1864-1873.
3. Hans Behrbohm, Oliver Kaschke, Andrew Swift. Ear, Nose and Throat Diseases,Thieme Stutgart 2009,311-313.
4. John Jacob Ballenger. Diseases of the Nose, Throat, Ear, Head and Neck, Lea&Febiger 1991,589-598.
5. Johnson JT. Laryngeal trauma. In :Mayers EN, editors. Operative Otolaryngology Head and Neck Surgery, Volume 1.Philadelphia:W.B.Saunders C ompany:1997. 345-347.
6. Nels R. Olson. English Otolaryngology, J.B.Lippincott Company 1992,1-13. Olson NR. Surgical treatment of acute blunt laryngeal injuries. Ann Oto| Rhino|Laryngo| 1978; 87:716-721.
7. Olson NR. Surgical treatment of acute blunt laryngeal injuries. Ann Oto| Rhino|Laryngo| 1978; 87:716-721.
8. Scott-Brown”s. Diseases of th ear, nose and throat. Butterworth&Co.Ltd.1971, 505-513.